Overview of Pediatric Leukemia
Leukemia is the most common cancer in children, accounting for about one-third of all pediatric cancer cases. It begins in the bone marrow—the spongy tissue inside bones where blood cells are produced—and results in the uncontrolled growth of abnormal white blood cells. These cells crowd out healthy ones, impairing the body’s ability to fight infection, carry oxygen, and control bleeding.
While leukemia can occur at any age, the disease behaves differently in children compared to adults. Pediatric leukemia not only differs in its biological makeup but also in how it responds to treatment and impacts long-term outcomes. Understanding these distinctions helps doctors provide better, more personalized care for children facing the diagnosis.
In most children, leukemia is highly treatable and even curable. Thanks to decades of research, survival rates for childhood leukemia now exceed 85%, a remarkable improvement compared to the past. However, the journey through diagnosis, treatment, and recovery remains uniquely challenging for young patients and their families.
Types of Leukemia in Children
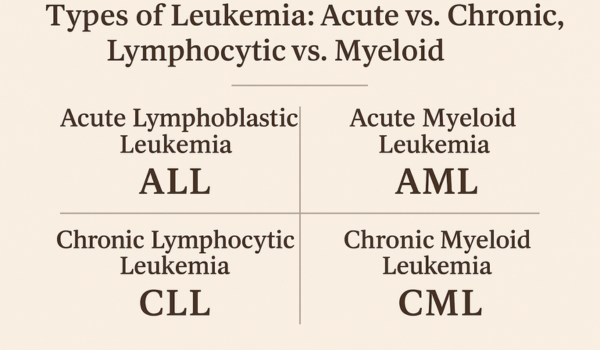
There are several forms of leukemia, but two types dominate in pediatric cases.
1. Acute Lymphoblastic Leukemia (ALL)
ALL is the most common childhood leukemia, representing nearly 75% of all cases. It develops from immature lymphoid cells—white blood cells that normally mature into B cells or T cells. ALL progresses rapidly and requires immediate treatment. Fortunately, it responds extremely well to modern chemotherapy, with survival rates over 90% in many cases.
2. Acute Myeloid Leukemia (AML)
AML accounts for about 20% of childhood leukemias. It originates in myeloid cells, which give rise to red blood cells, platelets, and other white cells. AML is more aggressive than ALL and can be more challenging to treat, but outcomes have steadily improved due to advances in bone marrow transplantation and targeted therapies.
Other rare pediatric types include Juvenile Myelomonocytic Leukemia (JMML) and Chronic Myeloid Leukemia (CML). These are less common and require specialized approaches.
How Pediatric Cases Differ from Adult Leukemia
The biological and clinical differences between pediatric and adult leukemia are profound. These differences influence treatment strategies, response rates, and long-term recovery.
1. Genetic and Molecular Profiles
Children’s leukemia often arises from different genetic mutations than adult cases. Pediatric ALL, for example, frequently involves rearrangements in genes like ETV6-RUNX1 or KMT2A, while adult leukemias often involve mutations linked to aging or environmental exposure. These distinctions mean that treatments effective in adults may not work the same way in children—and vice versa.
2. Treatment Tolerance
Children generally tolerate chemotherapy better than adults because their organs are younger and more resilient. This allows doctors to use more intensive regimens that eradicate cancer cells effectively. Adults, on the other hand, often have comorbidities—such as diabetes or heart disease—that limit how aggressive treatment can be.
3. Bone Marrow Response
Children’s bone marrow regenerates faster after chemotherapy, helping them recover blood counts more efficiently. This resilience contributes to their higher cure rates.
4. Long-Term Outlook
Pediatric leukemia often has a better prognosis, with cure rates exceeding 80% in many forms. In contrast, adult leukemias, especially acute myeloid leukemia (AML), have lower survival rates due to slower response and higher relapse risk.
Causes and Risk Factors
While leukemia’s exact cause remains uncertain, several factors are associated with increased risk in children.
-
Genetic syndromes such as Down syndrome, Li-Fraumeni syndrome, or Fanconi anemia raise leukemia susceptibility.
-
Prenatal factors, including maternal smoking or exposure to radiation during pregnancy, may slightly increase risk.
-
Environmental exposures like benzene or certain pesticides are being investigated as possible triggers.
-
Inherited genetic mutations play a more significant role in children than in adults, whose leukemias are more often linked to cumulative DNA damage from aging or lifestyle factors.
It’s important to note that most cases of childhood leukemia arise without any identifiable cause—meaning it cannot be prevented.
Signs and Symptoms
Because leukemia affects the blood and bone marrow, symptoms often mimic common childhood illnesses, making early detection challenging.
Typical symptoms include:
-
Persistent fatigue or weakness
-
Frequent infections or fevers
-
Easy bruising or bleeding (nosebleeds, gum bleeding, petechiae)
-
Bone or joint pain
-
Pale skin (anemia)
-
Swollen lymph nodes or abdomen (due to enlarged liver/spleen)
-
Loss of appetite and weight
Parents should consult a doctor if these symptoms persist or worsen over several weeks.
Diagnosis and Testing
Diagnosing pediatric leukemia requires a series of precise laboratory and imaging tests. The process begins with a complete blood count (CBC), which often reveals abnormal white blood cell counts or anemia. If leukemia is suspected, doctors perform:
-
Bone marrow aspiration and biopsy: to confirm leukemia cells in the bone marrow.
-
Immunophenotyping: to determine whether the leukemia is lymphoid (ALL) or myeloid (AML).
-
Cytogenetic and molecular testing: to identify gene mutations or chromosomal changes guiding treatment choices.
-
Lumbar puncture (spinal tap): to check if leukemia has spread to the central nervous system.
Early and accurate diagnosis helps clinicians choose the most effective therapy for each child’s leukemia type.
Treatment Approaches
Pediatric leukemia treatment has evolved dramatically, now focused on personalized, risk-based protocols that balance effectiveness with minimizing long-term toxicity.
1. Chemotherapy
Chemotherapy remains the cornerstone of treatment. It is typically delivered in multiple phases: induction (to achieve remission), consolidation (to destroy hidden leukemia cells), and maintenance (to prevent relapse). Modern chemotherapy protocols for children with ALL have pushed survival rates above 90%.
2. Targeted Therapy
Newer medications like tyrosine kinase inhibitors (TKIs)—used in children with Philadelphia chromosome-positive ALL or CML—block specific cancer-driving proteins. These drugs are far less toxic than traditional chemotherapy and improve survival.
3. Immunotherapy
Breakthroughs in immunotherapy are changing outcomes dramatically. Treatments like CAR T-cell therapy, which engineer a child’s immune cells to attack leukemia, are now approved for relapsed or refractory ALL. These therapies have shown long-lasting remissions in many children who previously had no remaining options.
4. Bone Marrow (Stem Cell) Transplantation
For high-risk cases or relapse, stem cell transplantation provides a potential cure. Healthy donor stem cells replace the damaged bone marrow after high-dose chemotherapy or radiation. Advances in donor matching and post-transplant care have improved survival and reduced complications.
5. Supportive Care
Treatment for leukemia is intense and can suppress the immune system. Supportive measures—such as antibiotics, blood transfusions, and nutritional support—are essential for safety and recovery.
Side Effects and Long-Term Risks
While modern treatments save lives, they can also cause short- and long-term side effects that must be carefully managed.
Short-Term Effects:
-
Nausea, vomiting, fatigue
-
Hair loss
-
Low blood counts (infection risk)
-
Mucositis (mouth sores)
Long-Term Risks:
-
Growth and hormone imbalances
-
Learning difficulties or neurocognitive effects
-
Fertility challenges
-
Increased risk of secondary cancers later in life
Because of these risks, survivors of childhood leukemia require long-term follow-up through specialized survivorship clinics to monitor and manage late effects.
Psychosocial and Emotional Support
A leukemia diagnosis affects not only the child but also their entire family. Emotional health plays a crucial role in overall recovery.
For the child:
Therapists and child-life specialists use play therapy, art, and counseling to help children express fear and anxiety.
For parents:
Support groups and social workers provide emotional guidance and practical resources during treatment. Financial and logistical assistance programs also help families manage costs and travel.
For siblings:
Brothers and sisters may feel overlooked or scared. Including them in conversations and care routines can strengthen family unity.
Survivorship and Life After Treatment
Most children treated for leukemia go on to live healthy, productive lives. However, survivorship doesn’t end when treatment stops—it continues with lifelong care and vigilance.
Regular follow-up visits monitor for recurrence and manage late effects.
Vaccinations and infection prevention remain vital as the immune system recovers.
Healthy lifestyle habits, such as balanced nutrition, physical activity, and avoiding tobacco exposure, help sustain long-term wellness.
The emotional transition from “cancer patient” to “survivor” also takes time. Many survivors and families benefit from counseling or support networks designed for pediatric cancer recovery.
Why Children Respond Better to Treatment
The remarkable success in pediatric leukemia stems from both biological and systemic factors:
-
Younger biology: Children’s rapidly dividing cells respond more readily to chemotherapy.
-
Fewer comorbidities: Unlike adults, children rarely have chronic conditions that complicate treatment.
-
Standardized care protocols: Global collaboration has led to evidence-based pediatric treatment guidelines.
-
Higher clinical trial participation: A large proportion of children receive care within research trials, ensuring access to cutting-edge therapy.
These advantages have made pediatric leukemia one of medicine’s greatest success stories in oncology.
Future Directions in Pediatric Leukemia Research
The future of childhood leukemia treatment looks even brighter, with ongoing studies focused on refining therapy and reducing long-term harm.
1. Genomic Medicine
Advances in genome sequencing are helping doctors classify leukemia more accurately, predict relapse risk, and tailor therapy to each child’s molecular profile.
2. Minimal Residual Disease (MRD) Monitoring
Sensitive tests that detect even one leukemia cell among a million normal cells allow doctors to fine-tune therapy and catch relapses earlier.
3. Novel Immunotherapies
Next-generation CAR T-cells, bispecific antibodies, and vaccines are under development to make immunotherapy safer, more durable, and accessible to more patients.
4. Reduced Toxicity Regimens
Researchers are designing gentler chemotherapy combinations and targeted drugs that preserve long-term health without compromising cure rates.
5. Psychosocial Health Integration
New care models emphasize the mental and emotional well-being of patients as part of comprehensive cancer care.
These breakthroughs aim not only to cure leukemia but to ensure survivors lead full, healthy lives free from major late effects.
.png)