Introduction
Leukemia is a cancer of the blood and bone marrow that arises when the body produces abnormal white blood cells. These cells multiply uncontrollably, crowding out healthy cells and disrupting normal blood function.
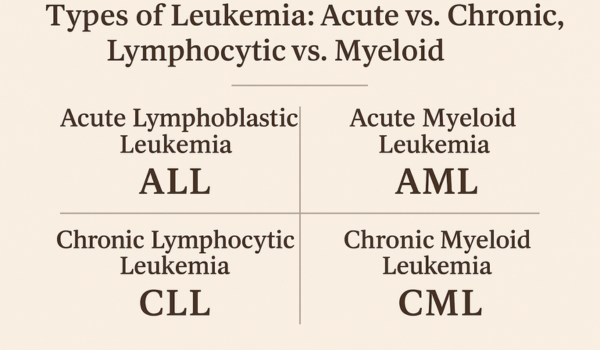
Doctors classify leukemia into four main categories, based on two key factors:
-
How quickly it progresses (acute vs. chronic).
-
The type of blood cell affected (lymphocytic vs. myeloid).
Understanding the differences between these types of leukemia is crucial for accurate diagnosis, treatment planning, and long-term outlook.
Acute vs. Chronic
Leukemia is first divided into acute or chronic forms depending on how rapidly the disease develops:
-
Acute leukemia:
-
Progresses quickly and requires immediate treatment.
-
Immature blood cells, known as blasts, accumulate rapidly.
-
Without intervention, acute leukemia can become life-threatening within weeks or months.
-
-
Chronic leukemia:
-
Develops slowly over years.
-
Involves more mature but abnormal white blood cells.
-
Patients may live with the condition for a long time before symptoms appear.
-
This distinction forms the foundation for understanding leukemia’s subtypes.
Lymphocytic vs. Myeloid
The second classification depends on which type of white blood cell is affected:
-
Lymphocytic (or lymphoblastic) leukemia:
-
Originates in lymphoid cells, which normally develop into B cells, T cells, or natural killer cells.
-
Impacts the immune system’s ability to fight infections.
-
-
Myeloid (or myelogenous) leukemia:
-
Starts in myeloid cells, which normally develop into red blood cells, platelets, and certain white cells like granulocytes.
-
Affects multiple blood cell types and often interferes with clotting and oxygen transport.
-
Combining these two classifications produces the four major types of leukemia.
Acute Lymphoblastic Leukemia (ALL)
ALL is the most common type of leukemia in children but can also affect adults.
Key features include:
-
Rapid accumulation of immature lymphoid cells.
-
Frequent infections, fatigue, and bleeding problems.
-
Bone pain and swollen lymph nodes are common early signs.
Risk factors:
-
Genetic syndromes such as Down syndrome.
-
Previous exposure to radiation or chemotherapy.
Treatment:
-
Multi-phase chemotherapy (induction, consolidation, maintenance).
-
Targeted therapy for specific genetic mutations.
-
Stem cell transplantation for high-risk or relapsed patients.
Children with ALL often respond better than adults, with cure rates exceeding 85%.
Acute Myeloid Leukemia (AML)
AML is most common in adults, especially those over 60, but it can occur at any age.
Key features include:
-
Rapid growth of abnormal myeloid cells.
-
Fatigue, frequent infections, bleeding, or bruising.
-
Pale skin and shortness of breath due to anemia.
Risk factors:
-
Long-term chemical exposure, especially benzene.
-
Prior chemotherapy or radiation therapy.
-
Genetic predispositions and chromosomal abnormalities.
Treatment:
-
Intensive chemotherapy to eliminate leukemia cells.
-
Targeted therapies like FLT3 inhibitors for patients with specific mutations.
-
Stem cell transplantation in eligible patients.
AML is aggressive and requires immediate treatment, but outcomes have improved with modern therapies.
Chronic Lymphocytic Leukemia (CLL)
CLL primarily affects older adults and is rare in children.
Key features include:
-
Slow accumulation of abnormal lymphocytes.
-
Many patients have no symptoms at diagnosis, discovered incidentally during routine blood tests.
-
Enlarged lymph nodes, fatigue, or frequent infections may develop later.
Risk factors:
-
Family history of CLL.
-
Certain genetic mutations or chromosomal abnormalities.
Treatment:
-
“Watch and wait” approach for patients without symptoms.
-
Targeted drugs such as BTK inhibitors (ibrutinib, acalabrutinib).
-
Monoclonal antibodies (rituximab) in combination regimens.
CLL is usually not curable, but many patients live for years with controlled disease.
Chronic Myeloid Leukemia (CML)
CML is characterized by the Philadelphia chromosome, which creates the BCR-ABL fusion gene. This abnormal gene drives uncontrolled growth of myeloid cells.
Key features include:
-
Often diagnosed in middle-aged adults.
-
Slow progression with a chronic phase, followed by an accelerated or blast crisis phase if untreated.
-
Symptoms include fatigue, night sweats, weight loss, and enlarged spleen.
Risk factors:
-
Primarily genetic changes, not lifestyle.
-
Exposure to high-dose radiation may increase risk.
Treatment:
-
Tyrosine kinase inhibitors (TKIs) such as imatinib, dasatinib, and nilotinib.
-
Stem cell transplantation for resistant or advanced cases.
TKIs have transformed CML from a fatal disease into a manageable chronic condition for most patients.
Other Rare Types
Beyond the four main subtypes, rare leukemias exist:
-
Hairy cell leukemia: A slow-growing form of chronic lymphocytic leukemia.
-
Mixed phenotype acute leukemia (MPAL): Shares characteristics of both lymphoid and myeloid leukemia.
-
Juvenile myelomonocytic leukemia (JMML): Rare pediatric leukemia affecting young children.
These rarer forms often require specialized treatment approaches.
Symptoms Across Types
While symptoms differ, many overlap among the leukemia subtypes:
-
Fatigue and weakness.
-
Frequent infections.
-
Easy bruising or bleeding.
-
Fever and night sweats.
-
Bone pain or swollen lymph nodes.
Acute leukemias typically present suddenly and severely, while chronic leukemias may remain silent for years.
Diagnosis
Doctors use several tests to identify leukemia type:
-
Blood tests: Reveal abnormal cell counts.
-
Bone marrow biopsy: Confirms leukemia and identifies subtype.
-
Genetic testing: Detects mutations like the Philadelphia chromosome.
-
Imaging scans: Evaluate organ involvement such as spleen or liver enlargement.
Accurate classification guides treatment decisions and prognosis.
Treatment Overview
Treatment depends on the leukemia type, patient age, and overall health:
-
Chemotherapy for acute leukemias.
-
Targeted therapy for genetic mutations such as BCR-ABL.
-
Immunotherapy including CAR-T cells and monoclonal antibodies.
-
Stem cell transplantation for high-risk patients.
-
Supportive care to manage infections, anemia, or side effects.
Research continues to refine therapies and reduce toxicity.
Prognosis
Prognosis varies widely between leukemia types:
-
ALL: High cure rates in children, lower in adults.
-
AML: Aggressive with variable outcomes, but improving with targeted drugs.
-
CLL: Often managed as a chronic condition, with many living decades.
-
CML: Excellent long-term outcomes with TKIs for most patients.
Early diagnosis and personalized treatment improve survival across all subtypes.
Future Directions
Advances in research are reshaping leukemia treatment:
-
Genomic medicine tailoring therapies to mutations.
-
Next-generation targeted therapies with fewer side effects.
-
Immunotherapy combinations to improve remission durability.
-
Artificial intelligence to predict relapse and guide therapy.
The future promises more effective, personalized care for all leukemia patients.
Conclusion
Leukemia is not one disease but a group of cancers with distinct patterns. By classifying it as acute or chronic, and lymphocytic or myeloid, doctors can identify four main types—ALL, AML, CLL, and CML—each with unique causes, symptoms, and treatments.
Understanding these differences empowers patients and families to seek timely medical help, make informed decisions, and embrace treatment with hope for long-term survival.

.png)