Introduction
Leukemia is a cancer of the blood and bone marrow that disrupts normal blood cell production. It begins when abnormal white blood cells grow uncontrollably, crowding out healthy red cells, platelets, and immune cells.
Because leukemia does not typically form solid tumors, diagnosing it can be more complex than diagnosing other cancers. Instead, doctors rely on a combination of physical exams, blood tests, bone marrow biopsies, and genetic studies to confirm the disease.
This article explains the key methods used to diagnose leukemia, the role of each test, and why early detection makes a difference.
Early Warning Signs
Diagnosis often begins with identifying potential symptoms:
-
Persistent fatigue or weakness.
-
Frequent infections.
-
Unexplained bruising or bleeding.
-
Swollen lymph nodes or enlarged spleen.
-
Night sweats, fever, or weight loss.
Because these symptoms overlap with common illnesses, further testing is necessary to confirm leukemia.
Physical Examination
The first step is usually a thorough physical exam. Doctors check for:
-
Enlarged lymph nodes in the neck, armpits, or groin.
-
Signs of anemia such as pale skin.
-
Bruises or small red spots (petechiae) that indicate bleeding problems.
-
An enlarged spleen or liver detected by abdominal palpation.
A physical exam cannot confirm leukemia but provides essential clues for ordering further tests.
Medical History
Doctors also review medical and family history:
-
Prior exposure to radiation or chemotherapy.
-
Occupational risks like benzene exposure.
-
Family history of blood cancers or genetic conditions.
-
Previous medical issues that may mimic or contribute to symptoms.
This background helps guide the choice of diagnostic tests.
Blood Tests
Blood tests are central to leukemia diagnosis and often the first step after suspicious symptoms appear.
-
Complete blood count (CBC): Measures levels of red blood cells, white blood cells, and platelets. Abnormal counts may suggest leukemia.
-
Blood smear: A slide examined under a microscope to identify abnormal or immature cells called “blasts.”
-
Biochemical tests: Assess organ function and rule out other causes of symptoms.
Abnormal results usually trigger a referral to a hematologist for specialized evaluation.
Bone Marrow Biopsy
The gold standard for confirming leukemia is a bone marrow biopsy.
-
Performed under local anesthesia, usually from the hip bone.
-
A needle extracts a sample of marrow for microscopic and genetic analysis.
-
Confirms whether abnormal cells are present, and how many.
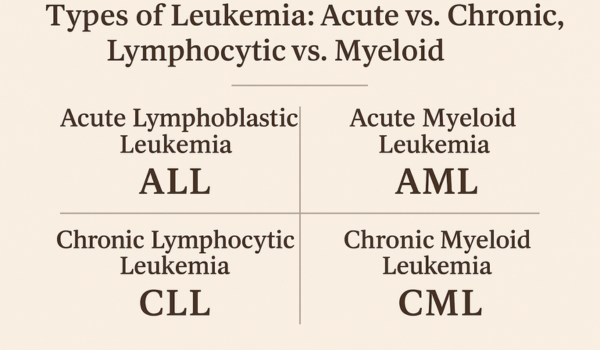
Bone marrow testing also helps determine the type of leukemia—acute or chronic, lymphocytic or myeloid.
Flow Cytometry
Flow cytometry is a powerful tool for classifying leukemia:
-
Analyzes proteins on the surface of blood or bone marrow cells.
-
Helps identify whether cells are lymphoid or myeloid in origin.
-
Differentiates between acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), and chronic myeloid leukemia (CML).
Precise classification is essential for selecting the right treatment.
Cytogenetic Testing
Cytogenetics examines chromosomes inside leukemia cells to detect abnormalities:
-
Karyotyping: Maps chromosomes under a microscope to reveal large structural changes.
-
FISH (fluorescence in situ hybridization): Uses fluorescent dyes to detect specific genetic abnormalities, like the Philadelphia chromosome in CML.
These tests identify mutations that influence treatment decisions and prognosis.
Molecular Testing
Advances in molecular biology allow detection of small but significant mutations:
-
PCR (polymerase chain reaction): Detects fusion genes such as BCR-ABL, which drives CML.
-
Next-generation sequencing (NGS): Provides a detailed genetic profile, uncovering mutations in FLT3, NPM1, and other genes.
-
Minimal residual disease (MRD) testing: Measures tiny amounts of leukemia cells remaining after treatment.
Molecular testing personalizes treatment by matching drugs to the genetic profile of leukemia cells.
Imaging Tests
While leukemia is primarily a blood cancer, imaging may be used to evaluate complications:
-
X-rays to check for infections or lung involvement.
-
CT scans or MRI to assess organ enlargement or nervous system spread.
-
Ultrasound to evaluate spleen or liver size.
Imaging supports staging and treatment planning, though it does not diagnose leukemia alone.
Lumbar Puncture
Also known as a spinal tap, this test checks whether leukemia has spread to the central nervous system.
-
A needle extracts cerebrospinal fluid (CSF) for analysis.
-
Commonly performed in patients with acute lymphoblastic leukemia (ALL).
-
Helps guide the need for intrathecal chemotherapy (treatment directly into CSF).
Differential Diagnosis
Doctors must rule out other conditions that mimic leukemia, such as:
-
Severe infections.
-
Vitamin deficiencies causing abnormal blood counts.
-
Autoimmune disorders.
-
Other cancers involving bone marrow.
Accurate diagnosis avoids unnecessary treatments and ensures the right therapy is started.
Children vs. Adults
Diagnosis may vary slightly depending on age:
-
Children: Rapid disease progression often makes diagnosis quicker. Genetic testing is emphasized to guide therapy.
-
Adults: Chronic forms may be detected incidentally on routine blood work. Additional testing is often needed to separate leukemia from other age-related conditions.
Age-specific protocols ensure patients receive the most appropriate care.
Importance of Early Detection
Early and accurate diagnosis provides several advantages:
-
Increases chances of effective treatment.
-
Allows doctors to start therapy before complications arise.
-
Improves survival rates, especially in acute leukemias.
-
Provides access to targeted therapies or clinical trials.
Awareness of early testing options empowers patients to seek timely medical help.
Future Advances
Leukemia diagnosis is evolving with cutting-edge research:
-
Liquid biopsies detecting cancer DNA in blood.
-
AI-driven analysis of blood smears and genetic data.
-
Point-of-care molecular testing for rapid diagnosis in clinics.
-
Global registries for better understanding of rare subtypes.
These innovations promise faster, more accurate, and less invasive diagnostic methods.
Conclusion
Diagnosing leukemia involves more than one test—it requires a careful combination of blood counts, bone marrow biopsy, flow cytometry, cytogenetics, and molecular testing.
While the process may feel overwhelming, each step provides critical information that shapes treatment. Early recognition of symptoms and timely diagnostic testing can make the difference between delayed treatment and a successful outcome.

.png)