Understanding Leukemia Treatment
Leukemia is a complex cancer of the blood and bone marrow that disrupts the body’s ability to produce healthy blood cells. Because it develops in the bloodstream rather than as a solid tumor, treatment focuses on eliminating abnormal cells throughout the body and restoring normal bone-marrow function.
Modern medicine offers several effective treatment options—ranging from traditional chemotherapy to cutting-edge targeted and immunotherapies.
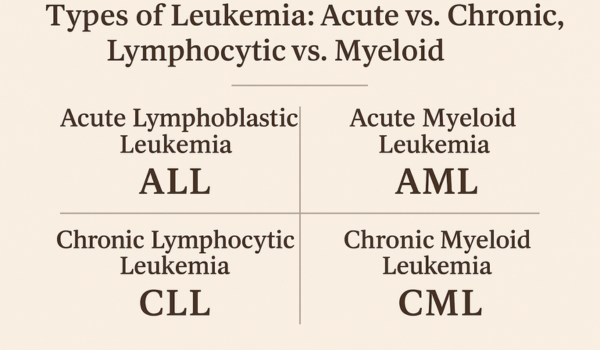
The right approach depends on the leukemia type (acute or chronic, lymphocytic or myeloid), disease stage, genetic markers, age, and overall health.
Chemotherapy
Chemotherapy remains the cornerstone of leukemia treatment. It uses potent drugs to destroy rapidly dividing cells, including the abnormal white blood cells that define leukemia.
1. How It Works
Chemotherapy circulates through the bloodstream, attacking leukemia cells wherever they are. Most regimens combine multiple drugs that act at different stages of cell division, maximizing effectiveness while preventing resistance.
2. Administration
-
Intravenous (IV) infusion through veins.
-
Oral pills for maintenance or chronic cases.
-
Intrathecal injection directly into cerebrospinal fluid to prevent spread to the brain and spinal cord.
3. Treatment Phases
-
Induction therapy: The first and most intense phase, aiming for remission by destroying visible leukemia cells.
-
Consolidation therapy: Eliminates hidden residual cells.
-
Maintenance therapy: Lower-dose regimens that keep the cancer from returning.
4. Common Drugs
-
Cytarabine (Ara-C)
-
Daunorubicin or Doxorubicin
-
Vincristine
-
Methotrexate
5. Side Effects
Because chemotherapy also harms normal cells, patients may experience fatigue, nausea, hair loss, mouth sores, and infection risk. Supportive care—anti-nausea medication, growth factors, and transfusions—helps manage these issues.
Targeted Therapy
Targeted therapy represents one of the greatest breakthroughs in leukemia treatment. Unlike chemotherapy, which attacks all rapidly dividing cells, targeted drugs block specific genetic or molecular changes that drive cancer growth.
1. Tyrosine Kinase Inhibitors (TKIs)
For chronic myeloid leukemia (CML) and some acute lymphoblastic leukemia (ALL) cases, TKIs block the abnormal BCR-ABL protein created by the Philadelphia chromosome.
Examples include:
-
Imatinib (Gleevec)
-
Dasatinib (Sprycel)
-
Nilotinib (Tasigna)
These agents can turn CML from a fatal disease into a manageable chronic condition.
2. FLT3 and IDH Inhibitors
Certain acute myeloid leukemia (AML) cases involve FLT3 or IDH mutations. Drugs like Midostaurin, Gilteritinib, Ivosidenib, and Enasidenib specifically target those proteins, improving remission rates and survival.
3. BCL-2 and BTK Inhibitors
For chronic lymphocytic leukemia (CLL), targeted drugs like Venetoclax (BCL-2 inhibitor) and Ibrutinib (BTK inhibitor) stop leukemia cells from avoiding programmed death, often replacing traditional chemo altogether.
4. Advantages
-
More precise and less toxic than chemotherapy
-
Often taken orally at home
-
May be combined with other therapies for long-term control
5. Limitations
Some patients eventually develop drug resistance, requiring new combinations or next-generation inhibitors.
Immunotherapy
Immunotherapy harnesses the patient’s immune system to find and destroy leukemia cells.
1. Monoclonal Antibodies
Lab-made antibodies recognize proteins on leukemia cells and mark them for immune attack.
Examples:
-
Rituximab (targets CD20, used in CLL and some ALL)
-
Ofatumumab and Obinutuzumab (enhanced anti-CD20 agents)
-
Blinatumomab (Blincyto), a bispecific T-cell engager that links immune cells to leukemia cells.
2. CAR T-Cell Therapy
This cutting-edge treatment involves genetically reprogramming a patient’s T cells to recognize and kill leukemia cells.
-
Approved for relapsed/refractory ALL and some lymphomas.
-
Patients’ blood is collected, T cells are modified in a lab, multiplied, and reinfused.
3. Immune Checkpoint Inhibitors
Still under research, these drugs release the immune system’s “brakes,” allowing stronger attacks on cancer cells.
4. Benefits and Challenges
CAR T-cell therapy and monoclonal antibodies can achieve long-lasting remission even in advanced disease, but they carry risks like cytokine release syndrome (CRS) and neurological effects that require specialized care.
Stem Cell Transplant
Stem cell (or bone marrow) transplantation offers the possibility of cure for many leukemia patients.
1. Purpose
It replaces the patient’s diseased bone marrow with healthy stem cells capable of producing normal blood cells.
2. Types of Transplant
-
Allogeneic transplant: Uses donor stem cells (most common for leukemia).
-
Autologous transplant: Uses patient’s own previously collected healthy cells (less common).
3. Process
After high-dose chemotherapy or radiation eliminates diseased marrow, donor stem cells are infused intravenously—similar to a blood transfusion. Over weeks, these cells repopulate the marrow with healthy new blood cells.
4. Risks and Complications
-
Graft-versus-host disease (GVHD)
-
Infection and bleeding during recovery
-
Organ toxicity due to intensive conditioning therapy
Despite risks, transplants remain the only curative option for many high-risk or relapsed leukemias.
Radiation Therapy
Radiation uses high-energy beams to kill leukemia cells or relieve specific symptoms.
1. Uses in Leukemia
-
To treat or prevent leukemia spread to the brain and spinal cord.
-
To shrink enlarged spleen or lymph nodes.
-
As part of pre-transplant conditioning.
2. Types
-
External beam radiation targets specific body areas.
-
Total body irradiation (TBI) is used before stem cell transplantation.
3. Side Effects
Fatigue, skin irritation, or nausea are common but temporary. Long-term effects depend on the radiation area and dose.
Clinical Trials and Emerging Therapies
Ongoing research continually reshapes leukemia care. Patients who join clinical trials gain access to novel therapies before they reach general use.
1. Experimental Treatments
-
Next-generation TKIs for resistant CML
-
Bispecific antibodies for refractory ALL
-
Gene-editing techniques (CRISPR) to correct faulty DNA sequences
2. Cancer Vaccines
Experimental vaccines train the immune system to recognize leukemia-specific antigens, reducing relapse risk after remission.
3. Personalized Medicine
Doctors now use molecular profiling to design customized therapy combinations, ensuring each patient receives the most effective, least toxic plan.
Supportive Care
Treatment success depends not only on anti-cancer drugs but also on managing side effects and maintaining quality of life.
1. Blood Transfusions
Used to treat anemia (low red cells) and thrombocytopenia (low platelets).
2. Growth Factors
Drugs like filgrastim (G-CSF) stimulate white cell recovery after chemotherapy.
3. Antibiotics and Antivirals
Prevent or treat infections due to weakened immunity.
4. Nutrition and Mental Health
Healthy diet, physical activity, and counseling improve resilience and long-term well-being.
Choosing the Right Treatment
Decisions about treatment depend on multiple factors:
-
Leukemia type and genetic mutations
-
Age and fitness level
-
Stage or phase at diagnosis
-
Presence of comorbidities (heart, kidney, or liver disease)
-
Patient preference and lifestyle
A multidisciplinary team—hematologists, oncologists, nurses, nutritionists, and psychologists—collaborates to design the best approach. Some treatments aim for cure, others for long-term control or symptom relief.
Combination Approaches
In many cases, doctors combine therapies to achieve better outcomes:
-
Chemo + Targeted Therapy: For example, adding imatinib to chemotherapy in Philadelphia-positive ALL.
-
Chemo + Immunotherapy: Rituximab with fludarabine or cyclophosphamide for CLL.
-
Transplant + Maintenance Therapy: Targeted or immune drugs to prevent relapse after transplant.
Such multi-modal strategies are helping transform leukemia from an often-fatal disease into a chronic, manageable condition.
Managing Side Effects
Leukemia treatments can strain the body, but modern medicine offers many tools to help patients cope.
-
Nausea and appetite loss: Anti-emetics and nutritional support.
-
Hair loss: Usually temporary; wigs or scarves help maintain confidence.
-
Fatigue: Rest, light exercise, and mental-health care.
-
Mouth sores: Special rinses and soft diets.
-
Emotional distress: Support groups and therapy sessions.
Regular monitoring ensures complications are caught early and managed effectively.
Outlook and Survival
Survival rates have improved dramatically:
-
ALL: Up to 90% cure rate in children; 40%–60% in adults.
-
AML: 25%–40% long-term survival after remission.
-
CML: Over 90% 5-year survival with TKIs.
-
CLL: Many patients live over 10–15 years, especially with targeted therapy.
Early diagnosis, molecular testing, and continued innovation continue to improve these outcomes every year.
Future Directions
The future of leukemia treatment lies in precision medicine and immune engineering.
-
Artificial intelligence (AI) helps identify genetic mutations faster.
-
CAR-NK (natural killer) cells may offer safer immune therapies.
-
Microbiome research explores how gut health influences treatment success.
With ongoing progress, the goal is not just remission—but a cure without long-term toxicity.
Conclusion
From chemotherapy to targeted and immune-based therapies, leukemia treatment has evolved into a highly personalized science.
Patients today benefit from options that are safer, more effective, and better tailored to their disease profile.
Whether through conventional regimens or advanced genetic therapies, every approach brings us one step closer to making leukemia a fully curable disease.

.png)