Understanding Leukemia Progression
Leukemia is a cancer of the blood and bone marrow that disrupts the body’s ability to produce healthy blood cells. Unlike many cancers that form solid tumors, leukemia involves abnormal white blood cells that multiply uncontrollably.
Because of this, its “staging” system differs from those used for other cancers. Instead of describing the tumor’s size or spread, leukemia stages describe the severity of the disease, how much bone marrow or blood is affected, and how the abnormal cells impact overall health.
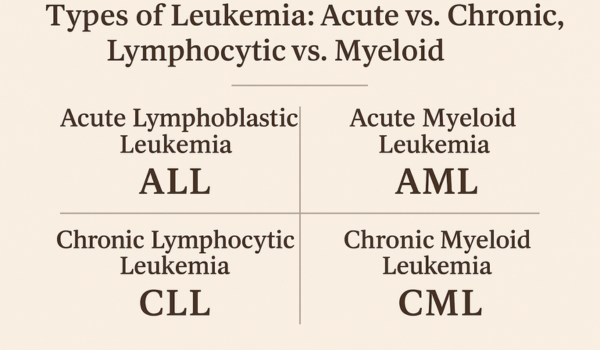
Leukemia is broadly classified into four major types — acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), acute myeloid leukemia (AML), and chronic myeloid leukemia (CML).
Each type progresses differently and has unique staging or phase systems. Understanding these stages is vital for predicting outcomes and choosing the most effective treatment.
Acute vs. Chronic Leukemia
The most basic way to stage leukemia begins with how fast it develops:
-
Acute leukemia progresses rapidly. The abnormal cells are immature and unable to function properly, causing symptoms to appear quickly and worsen within weeks or months if untreated.
-
Chronic leukemia progresses slowly. The abnormal white cells may still function for some time, allowing patients to live with mild or no symptoms for years before the disease advances.
This distinction determines the urgency and type of treatment. Acute leukemia requires immediate intervention, while chronic forms may be monitored under “watchful waiting” before therapy begins.
Staging in Acute Lymphoblastic Leukemia (ALL)
Acute lymphoblastic leukemia is the most common leukemia in children but can also affect adults.
ALL staging focuses less on “numbered stages” and more on risk categories based on lab results, age, and response to therapy.
1. Initial Diagnosis and Blast Count
At diagnosis, doctors evaluate the number of blast cells—immature white blood cells—in the bone marrow.
If more than 20% of the bone marrow cells are blasts, the condition qualifies as leukemia.
2. Risk-Based Grouping
Instead of stages, patients are classified into:
-
Standard-risk (low-risk): Younger patients (typically under 10 years), white blood cell count below 50,000/μL, and rapid response to initial treatment.
-
High-risk: Older patients, higher white blood cell counts, or slower response to therapy.
-
Very high-risk: Specific chromosomal abnormalities such as the Philadelphia chromosome (BCR-ABL1) or early relapse.
3. Treatment Phases
Doctors divide treatment into phases:
-
Induction phase: First 4–6 weeks, aiming to eliminate most leukemia cells and induce remission.
-
Consolidation (intensification): Prevents regrowth and addresses cells hiding in the brain or spinal fluid.
-
Maintenance: Lower-dose therapy to keep leukemia from returning.
Remission doesn’t mean “cure” but signals that no leukemia cells are detectable under a microscope.
Stages in Acute Myeloid Leukemia (AML)
Acute myeloid leukemia, common among adults, progresses rapidly and affects myeloid cells that normally produce red cells, platelets, and some white cells.
1. Classification by Cell Type
AML is categorized based on the specific type of myeloid cell involved. The French-American-British (FAB) system once classified AML from M0 to M7, each describing different cell lineages.
2. Genetic and Molecular Staging
Today, AML is staged by genetic and chromosomal changes, as they strongly influence prognosis:
-
Favorable risk: Mutations such as NPM1, CEBPA, or RUNX1 with normal chromosomes.
-
Intermediate risk: Some chromosomal irregularities, moderate treatment response.
-
Adverse risk: Complex or unfavorable genetic profiles, like deletions of chromosomes 5 or 7, or TP53 mutations.
3. Disease Status
AML stages also describe response to treatment:
-
Newly diagnosed: Active leukemia in blood or bone marrow.
-
Remission: Less than 5% blasts, normal blood counts.
-
Relapsed: Leukemia cells reappear after remission.
-
Refractory: Leukemia resists initial treatment.
Each status influences the next step—additional chemotherapy, targeted therapy, or stem cell transplant.
Chronic Lymphocytic Leukemia (CLL) Staging
Chronic lymphocytic leukemia progresses slowly, and most staging systems rely on blood counts and lymph node enlargement rather than microscopic blast percentage.
1. Rai Staging System (Used in the U.S.)
This system divides CLL into five stages:
-
Stage 0: Only increased lymphocytes in blood and bone marrow.
-
Stage I: Enlarged lymph nodes.
-
Stage II: Enlarged liver or spleen.
-
Stage III: Low red blood cell count (anemia).
-
Stage IV: Low platelet count (thrombocytopenia).
Stages 0–II are “early or intermediate,” while III–IV indicate “advanced disease.”
2. Binet System (Used in Europe)
CLL is divided into Stage A, B, and C:
-
A: Fewer than three lymphoid areas (neck, groin, spleen) enlarged.
-
B: Three or more enlarged lymphoid areas.
-
C: Low red blood cells or platelets.
3. What These Mean for Patients
Early-stage CLL may require only monitoring, known as watchful waiting, since immediate treatment doesn’t improve survival.
However, when symptoms like fatigue, weight loss, night sweats, or blood count drops appear, treatment with targeted drugs or monoclonal antibodies begins.
Phases of Chronic Myeloid Leukemia (CML)
Chronic myeloid leukemia has a unique staging model because it progresses through distinct biological phases driven by the Philadelphia chromosome (BCR-ABL fusion gene).
1. Chronic Phase
-
Typically, 90% of diagnoses occur in this phase.
-
Patients may be asymptomatic or have mild symptoms (fatigue, fullness in abdomen).
-
Fewer than 10% of cells in bone marrow are blasts.
-
Responds well to tyrosine kinase inhibitors (TKIs) such as imatinib or dasatinib.
2. Accelerated Phase
-
Blasts increase to 10–19% in blood or marrow.
-
Enlarged spleen, anemia, or higher white blood cell count despite treatment.
-
This phase signals loss of disease control and may require stronger or combination therapies.
3. Blast Crisis Phase
-
The most aggressive stage, with 20% or more blasts.
-
Resembles acute leukemia, often resistant to treatment.
-
Patients may need stem cell transplantation after attempting to regain control with TKIs or chemotherapy.
The goal is to keep CML in the chronic phase as long as possible through ongoing targeted therapy.
Other Factors That Affect Staging
Leukemia staging isn’t based on tumor spread, but several prognostic indicators influence how doctors classify disease severity:
-
Cytogenetic abnormalities: Specific DNA changes predict how leukemia behaves.
-
White blood cell count: Higher counts usually mean more aggressive disease.
-
Age and overall health: Older patients often tolerate treatment less effectively.
-
Response to initial therapy: Rapid remission signals better outlook.
-
Central nervous system involvement: Presence of leukemia in spinal fluid marks advanced disease.
How Stages Guide Treatment Decisions
Understanding leukemia stages helps doctors:
-
Select the right therapy: For example, targeted drugs for CML, intensive chemo for AML.
-
Determine treatment timing: Some early-stage CLL patients can delay therapy safely.
-
Estimate prognosis: Certain genetic markers indicate likelihood of remission or relapse.
-
Plan for transplant: Advanced or recurrent leukemia may require bone marrow transplant.
For patients, staging also helps them mentally prepare for what lies ahead—whether it’s months of chemotherapy or long-term monitoring with pills.
Remission and Relapse
After treatment, patients enter remission when leukemia cells are no longer detectable in tests.
However, minimal residual disease (MRD)—tiny traces of cancer cells—can remain. MRD monitoring via molecular tests helps detect relapse early, often before symptoms reappear.
Relapse means leukemia has returned. It can happen in blood, bone marrow, or, rarely, in the brain or spinal cord.
Treatment depends on the type and prior response but may involve different chemotherapy combinations, targeted therapy, or a stem cell transplant.
Prognosis by Stage
Leukemia survival rates have improved dramatically due to better diagnostics and targeted therapies. Prognosis varies:
-
ALL: 90% cure rate in children, ~40% in adults.
-
AML: 60–70% remission after initial therapy; 25–40% long-term survival.
-
CLL: Median survival over 10 years for early-stage disease.
-
CML: Over 90% five-year survival in chronic phase with TKIs.
Earlier detection and newer therapies continue to extend life expectancy and quality of life for patients in all stages.
Living Through Different Stages
Each stage or phase comes with emotional and physical challenges.
In early stages, uncertainty and anxiety are common; in advanced phases, fatigue, infections, or bleeding risks increase.
Support systems—family, psychological counseling, and patient communities—help individuals navigate treatment and recovery.
Patients are encouraged to:
-
Maintain balanced nutrition.
-
Follow medication schedules strictly.
-
Monitor side effects closely.
-
Engage in light activity to preserve strength.
-
Communicate openly with healthcare providers about mental well-being.
Future Outlook
The future of leukemia care is promising.
Advancements in genetic testing, immunotherapy, and personalized medicine are transforming how doctors stage and treat the disease.
Instead of relying only on microscope observations, doctors can now sequence DNA to predict relapse risk and tailor therapy accordingly.
Emerging treatments like CAR T-cell therapy, bispecific antibodies, and next-generation TKIs offer hope even for advanced stages that were once untreatable.
Research continues toward making leukemia a fully manageable chronic disease—and ultimately, curable.
Conclusion
Understanding the stages of leukemia helps both doctors and patients make informed decisions.
Whether acute or chronic, lymphoid or myeloid, each type follows its own path—but with today’s medical progress, even advanced stages are no longer hopeless.
Knowledge empowers patients to face their diagnosis with clarity and confidence, turning fear into proactive care.

.png)