.png)
Pancreatic cancer is not a single disease, but rather a group of malignancies that originate in different types of cells within the pancreas. Understanding the types of pancreatic cancer is essential for diagnosis, treatment, and prognosis. The two major categories of pancreatic cancer are exocrine tumors and pancreatic neuroendocrine tumors (PNETs), also known as endocrine tumors. Each type behaves differently, responds to treatment in unique ways, and carries a distinct prognosis.
This article provides a comprehensive overview of exocrine and neuroendocrine pancreatic cancers—their origins, characteristics, risk factors, symptoms, and treatment options—to help patients, caregivers, and healthcare providers better understand this complex disease.
Overview of Pancreatic Anatomy and Function
The pancreas is a glandular organ located deep in the abdomen, behind the stomach. It performs two major functions:
-
Exocrine function: Produces digestive enzymes that are secreted into the small intestine through ducts. These enzymes help digest proteins, fats, and carbohydrates.
-
Endocrine function: Produces hormones such as insulin and glucagon, which regulate blood sugar levels. These hormones are released directly into the bloodstream.
Depending on where cancer arises—either in the exocrine or endocrine cells—patients may experience different symptoms and require different treatments.
Exocrine Pancreatic Cancer
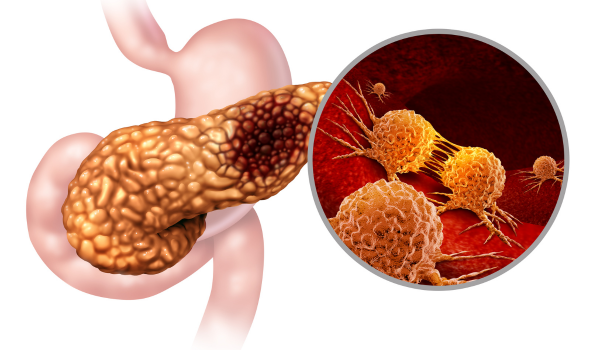
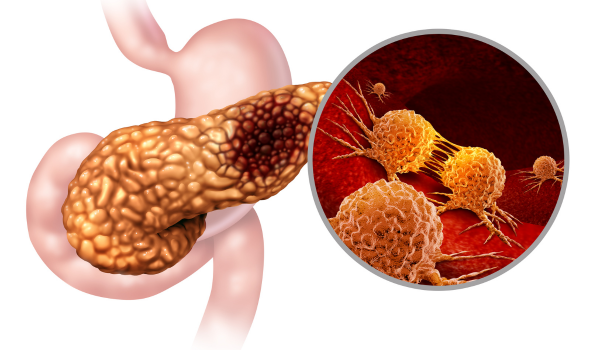
Exocrine tumors are by far the most common form of pancreatic cancer, accounting for more than 90% of all cases. These cancers typically begin in the ducts that carry digestive enzymes and are collectively referred to as pancreatic ductal adenocarcinoma (PDAC).
1. Pancreatic Ductal Adenocarcinoma (PDAC) PDAC is the most aggressive and lethal form of pancreatic cancer. It typically begins in the lining of the pancreatic ducts and has a high potential for invasion and metastasis. Most patients with PDAC are diagnosed at an advanced stage, as early symptoms are often minimal or nonspecific.
2. Acinar Cell Carcinoma This rare subtype originates from the enzyme-producing cells of the pancreas (acinar cells). While still aggressive, it may have slightly different features and behavior compared to ductal adenocarcinoma.
3. Adenosquamous Carcinoma and Other Rare Variants Adenosquamous carcinoma contains both glandular and squamous cell elements and tends to be particularly aggressive. Other rare exocrine tumors include colloid carcinoma, hepatoid carcinoma, and undifferentiated carcinoma.
Symptoms of Exocrine Pancreatic Cancer:
-
Jaundice (yellowing of the skin and eyes)
-
Abdominal or back pain
-
Unexplained weight loss
-
Loss of appetite
-
Fatigue
-
Digestive problems such as nausea or greasy stools (steatorrhea)
These symptoms often appear after the cancer has progressed, making early detection difficult.
Risk Factors for Exocrine Tumors:
-
Smoking
-
Chronic pancreatitis
-
Long-standing diabetes
-
Obesity
-
Family history or genetic syndromes (BRCA mutations, Lynch syndrome)
Diagnosis and Treatment of Exocrine Tumors: Diagnosis typically involves imaging (CT, MRI, or EUS), blood tests for tumor markers like CA 19-9, and a biopsy. Treatment often includes surgery (if operable), chemotherapy, radiation, or palliative care in advanced cases. The Whipple procedure is the most common surgical approach for tumors in the head of the pancreas.
Unfortunately, the prognosis for PDAC is poor, with a five-year survival rate below 12%, due to late detection and rapid progression.
Pancreatic Neuroendocrine Tumors (PNETs)
Neuroendocrine tumors arise from the hormone-producing cells of the pancreas. They are far less common than exocrine tumors, accounting for around 5–10% of all pancreatic cancers. PNETs tend to grow more slowly and may have a more favorable prognosis, especially if diagnosed early.
PNETs are categorized as either functional or non-functional depending on whether they produce excess hormones:
1. Functional PNETs These tumors produce hormones that cause recognizable clinical syndromes:
-
Insulinomas: Produce insulin, leading to episodes of low blood sugar (hypoglycemia).
-
Gastrinomas: Produce gastrin, causing Zollinger-Ellison syndrome (excess stomach acid and ulcers).
-
Glucagonomas: Cause high blood sugar and skin rashes.
-
VIPomas: Lead to watery diarrhea and electrolyte imbalances.
-
Somatostatinomas: May cause diabetes, gallstones, and digestive issues.
2. Non-functional PNETs These tumors do not produce active hormones and often grow silently until they are large enough to cause symptoms by compressing nearby structures.
Symptoms of PNETs:
-
Abdominal discomfort or fullness
-
Changes in blood sugar (for functional tumors)
-
Diarrhea or weight loss
-
Flushing or skin rash (in rare cases)
-
Tumor-related mass effects, such as jaundice or pain
Risk Factors for PNETs:
-
Genetic syndromes such as Multiple Endocrine Neoplasia type 1 (MEN1), von Hippel-Lindau syndrome, and tuberous sclerosis
-
Family history of neuroendocrine tumors
Diagnosis and Treatment of PNETs: Diagnosis often involves imaging (CT, MRI, somatostatin receptor PET scan), hormonal blood tests, and biopsy. Treatment options may include:
-
Surgical resection (potentially curative for localized tumors)
-
Targeted therapies (e.g., everolimus, sunitinib)
-
Somatostatin analogs (to control hormone-related symptoms)
-
Chemotherapy (for advanced or aggressive tumors)
-
Peptide receptor radionuclide therapy (PRRT)
Prognosis for PNETs is generally better than for exocrine tumors, with survival rates significantly higher, especially when tumors are functional and localized.
Key Differences Between Exocrine and Neuroendocrine Pancreatic Cancers
While both types of pancreatic cancer arise in the same organ, they are fundamentally different in their biology, presentation, and treatment:
-
Prevalence: Exocrine tumors are far more common.
-
Aggressiveness: Exocrine cancers, especially PDAC, tend to be more aggressive.
-
Symptoms: PNETs may present with hormone-related symptoms; exocrine tumors often cause jaundice and digestive issues.
-
Treatment response: PNETs may respond better to targeted and hormonal therapies.
-
Prognosis: PNETs generally have a more favorable prognosis.
Understanding these differences is essential for guiding treatment and setting realistic expectations for outcomes.
Conclusion
Pancreatic cancer is a heterogeneous disease with two major types: exocrine tumors and neuroendocrine tumors. Each has distinct characteristics, clinical presentations, and treatment strategies. While exocrine cancers are more common and typically more lethal, neuroendocrine tumors can often be managed more effectively, especially when detected early.
Awareness of the different types of pancreatic cancer empowers patients and healthcare professionals to pursue timely evaluations and tailor treatment plans accordingly. As research continues to advance in understanding the molecular biology of pancreatic tumors, there is growing hope for more precise therapies and improved survival for patients affected by this devastating disease.

.png)



.png)






