.png)
Pancreatic cancer is widely recognized not only for its aggressiveness and poor prognosis but also for the severe physical and emotional burden it places on patients. One of the most debilitating aspects of this disease is the high prevalence of pain and discomfort. Effective pain and symptom management is therefore a critical component of pancreatic cancer care. It not only improves quality of life but also enhances the patient’s ability to cope with treatment and maintain dignity throughout the course of the illness.
This article offers a comprehensive overview of the causes of pain in pancreatic cancer, common symptoms, and a multidisciplinary approach to managing them through medication, supportive therapies, and psychosocial care.
The Nature of Pain in Pancreatic Cancer
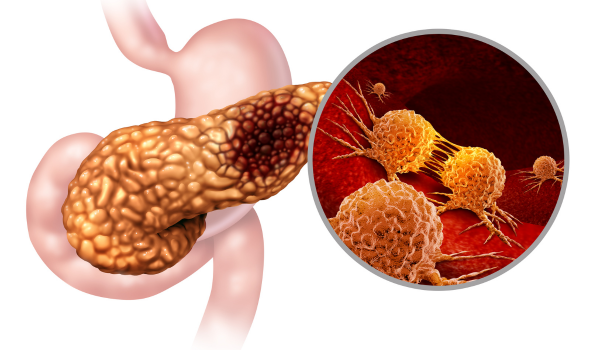
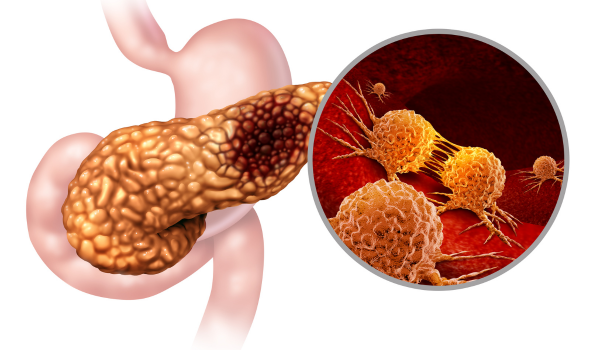
Pain in pancreatic cancer typically arises from several sources. As the tumor grows, it may invade nearby nerves, organs, or tissues, leading to persistent and sometimes severe abdominal or back pain. Tumors in the body or tail of the pancreas are more likely to cause back pain, while those in the head of the pancreas may obstruct the bile duct, leading to jaundice and associated discomfort.
Surgical interventions, chemotherapy, and radiation therapy can also contribute to pain or exacerbate existing symptoms. Furthermore, treatment side effects—such as nausea, neuropathy, fatigue, and digestive disturbances—can compound the patient’s overall discomfort.
Understanding the origin and type of pain is essential for tailoring an effective pain management strategy.
Common Symptoms Requiring Management
In addition to pain, pancreatic cancer is associated with a range of distressing symptoms that may include:
-
Nausea and vomiting
-
Loss of appetite and weight loss
-
Fatigue
-
Constipation or diarrhea
-
Jaundice (yellowing of the skin and eyes)
-
Ascites (fluid buildup in the abdomen)
-
Shortness of breath (particularly in advanced cases)
-
Emotional distress, depression, and anxiety
Each of these symptoms can significantly diminish quality of life and may require individualized interventions.
Principles of Pain Management
The World Health Organization (WHO) has developed a three-step analgesic ladder for cancer pain management that is widely adopted in clinical practice:
-
Mild Pain: Non-opioid medications such as acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs)
-
Moderate Pain: Addition of weak opioids like tramadol or codeine
-
Severe Pain: Strong opioids such as morphine, oxycodone, or fentanyl
Pain medications are often combined with adjuvant drugs to enhance efficacy and manage side effects. These include antidepressants, anticonvulsants (e.g., gabapentin), corticosteroids, and muscle relaxants.
Advanced Pain Control Techniques
When conventional medications are insufficient, more advanced interventions may be necessary:
-
Celiac Plexus Block: A minimally invasive procedure that involves injecting anesthetic into the nerves behind the pancreas to relieve chronic abdominal and back pain. It can offer long-lasting relief and reduce the need for high-dose opioids.
-
Radiation Therapy: Targeted radiation can shrink tumors that are pressing on nerves or organs, alleviating pain in the affected areas.
-
Palliative Surgery or Stenting: Surgical procedures or placement of stents can relieve symptoms caused by obstruction of bile ducts or the gastrointestinal tract.
-
Nerve Ablation or Neuromodulation: In certain cases, destruction or modulation of specific nerves responsible for pain transmission may be considered.
Managing Other Physical Symptoms
Effective care for pancreatic cancer extends beyond pain relief. Common symptoms are addressed as follows:
-
Nausea and Vomiting: Often managed with antiemetics such as ondansetron or metoclopramide. Dietary adjustments and hydration support also help.
-
Appetite Loss and Weight Loss: Nutritional counseling, appetite stimulants, and pancreatic enzyme replacement therapy may be employed to support intake and digestion.
-
Constipation: This is often related to opioid use or reduced mobility. Stool softeners, laxatives, and dietary fiber can help restore bowel regularity.
-
Diarrhea: Can be linked to malabsorption or infections. Antidiarrheal medications and enzyme replacement can provide relief.
-
Fatigue: Managed through energy conservation techniques, gentle physical activity, and addressing underlying causes like anemia or sleep disruption.
-
Jaundice: Caused by bile duct blockage, it is typically treated with stent placement or bypass surgery to restore bile flow.
-
Ascites: Paracentesis (fluid drainage) and diuretics may be used to relieve abdominal pressure and discomfort.
-
Shortness of Breath: Treated by addressing underlying causes such as fluid accumulation, infection, or anemia. Oxygen therapy and breathing exercises can offer additional support.
Psychological and Emotional Support
Pain and discomfort are not limited to the body; they often come with emotional and psychological distress. Anxiety, depression, and fear are common among pancreatic cancer patients and their families. Addressing these issues is essential to holistic care.
-
Psychological Counseling: Access to therapists or psychologists can help patients process emotions and develop coping strategies.
-
Support Groups: Connecting with others facing similar challenges can reduce feelings of isolation and provide practical advice.
-
Mind-Body Therapies: Techniques like mindfulness, meditation, guided imagery, and gentle yoga may reduce stress and improve pain perception.
-
Spiritual Care: Chaplaincy or faith-based counseling can provide comfort and meaning for patients experiencing existential distress.
The Role of Palliative and Hospice Care
Palliative care focuses on symptom management, emotional support, and quality of life at any stage of illness. It can be integrated early in the cancer journey and works alongside curative or life-prolonging treatments.
Hospice care, a subset of palliative care, is appropriate when the focus shifts entirely to comfort during the final months of life. Both approaches emphasize dignity, autonomy, and relief from suffering.
Early referral to palliative care teams has been shown to improve symptom control, patient satisfaction, and even survival in some cancer types.
Caregiver Involvement and Communication
Family caregivers play a vital role in symptom management, medication adherence, and emotional support. Educating caregivers about medication schedules, symptom monitoring, and communication with healthcare teams can empower them and reduce stress.
Regular and honest communication between patients, families, and providers ensures that care remains aligned with patient values and goals. Advanced care planning, including discussions about resuscitation preferences and end-of-life wishes, is a key component of comprehensive care.
Conclusion
Managing pain and discomfort in pancreatic cancer requires a compassionate, multidisciplinary approach that recognizes the complexity of the disease and the humanity of those affected by it. Through a combination of pharmacological treatments, supportive therapies, and emotional care, healthcare providers can greatly improve the day-to-day experience of patients.
Ultimately, effective symptom management is not just about relieving pain—it is about preserving dignity, fostering connection, and providing comfort during one of life’s most difficult journeys. As awareness and research grow, so too does the potential to enhance the lives of those living with pancreatic cancer and to bring relief where it is most needed.

.png)



.png)






