.png)
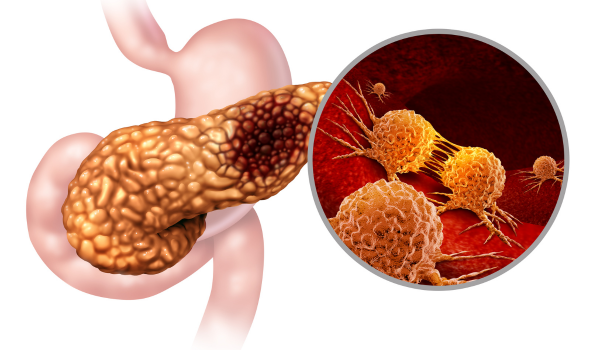
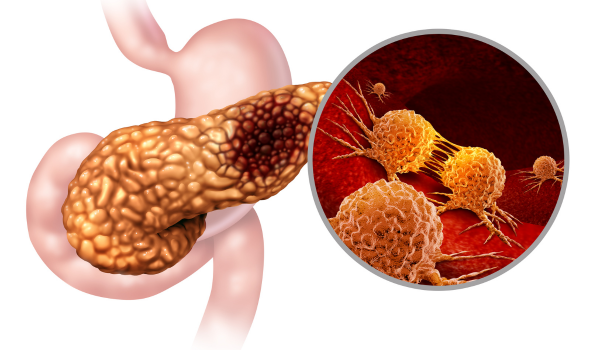
Pancreatic cancer is a complex and aggressive disease that often progresses silently in its early stages. By the time it is diagnosed, the cancer has frequently grown beyond the pancreas, making treatment more difficult. Understanding how pancreatic cancer develops in the body—from the initial cellular mutations to local invasion and metastasis—is crucial for improving early detection and advancing targeted therapies.
This article outlines the biological processes behind pancreatic cancer development, including genetic mutations, cellular changes, tumor growth, and how the cancer spreads to other parts of the body.
The Structure and Function of the Pancreas
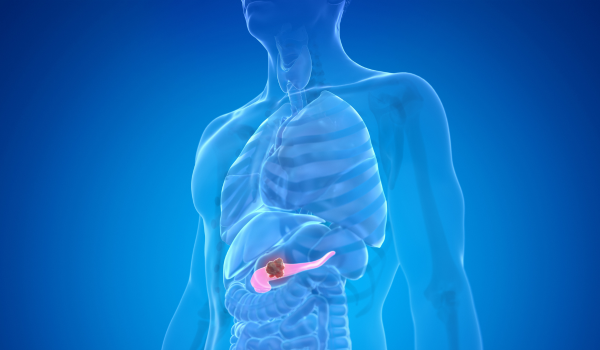
The pancreas is a glandular organ located deep within the abdomen, behind the stomach and near the small intestine. It has two primary functions:
-
Exocrine function: Produces digestive enzymes that are released into the small intestine to help break down food.
-
Endocrine function: Produces hormones like insulin and glucagon that regulate blood sugar levels.
Pancreatic cancer can develop in either component of the pancreas. Most commonly, it arises from the exocrine cells that line the ducts of the pancreas, which transport digestive enzymes. Less frequently, cancer originates from the hormone-producing endocrine cells, forming neuroendocrine tumors.
Cellular Mutation and DNA Damage
Like most cancers, pancreatic cancer begins at the cellular level. Healthy cells grow, divide, and die in an orderly process. Cancer starts when certain cells undergo mutations in their DNA, altering genes that control cell growth and division.
In pancreatic cancer, these mutations may occur spontaneously or be triggered by risk factors such as smoking, chronic inflammation (pancreatitis), obesity, diabetes, or inherited genetic mutations. These genetic changes can lead to:
-
Uncontrolled cell division: Mutations in oncogenes (genes that promote cell growth) become overactive.
-
Loss of tumor suppression: Tumor suppressor genes, such as TP53 and CDKN2A, which normally control cell division and repair DNA damage, may be turned off or deleted.
-
Evasion of cell death: Damaged cells that would normally die by apoptosis (programmed cell death) continue to survive and multiply.
As these abnormal cells accumulate, they may form a small tumor, often referred to as a pancreatic intraepithelial neoplasia (PanIN), which is considered a precursor to invasive pancreatic cancer.
From Pre-cancer to Malignancy
PanIN lesions can exist in the pancreas for years without causing noticeable symptoms. These early lesions are typically microscopic and confined to the ductal epithelium, the tissue lining the pancreatic ducts.
Over time, additional genetic alterations can drive these cells from low-grade dysplasia (abnormal development) to high-grade dysplasia and eventually to invasive pancreatic ductal adenocarcinoma (PDAC). This progression is characterized by:
-
Increased cell proliferation
-
Invasion through the basement membrane into nearby tissues
-
Recruitment of blood vessels (angiogenesis) to nourish the growing tumor
-
Avoidance of immune system detection
Once the tumor breaks through normal tissue boundaries, it is considered invasive cancer and can begin to affect the function of the pancreas and surrounding organs.
Tumor Microenvironment and Immune Evasion
As pancreatic cancer develops, it alters the surrounding tissue environment, known as the tumor microenvironment. This includes not only cancer cells but also immune cells, fibroblasts, blood vessels, and extracellular matrix.
The tumor microenvironment in pancreatic cancer is particularly dense and fibrotic, a condition known as desmoplasia. This can:
-
Create a physical barrier to immune cells and chemotherapy drugs
-
Promote further tumor growth through inflammatory signaling
-
Suppress normal immune responses by recruiting regulatory immune cells
Pancreatic tumors are also known for being immunologically “cold,” meaning they do not provoke a strong immune response. This helps them avoid detection and destruction by the body’s natural defenses.
Invasion and Local Spread
As the tumor expands, it begins to invade nearby structures within the abdomen. The pancreas is in close proximity to several vital organs and blood vessels, which allows cancer to spread locally before it causes symptoms.
Local invasion can affect:
-
The bile duct, leading to jaundice
-
The stomach or duodenum, causing digestive issues
-
Major blood vessels, which may make surgical removal difficult or impossible
-
Nerve plexuses, leading to back or abdominal pain
This early local invasion is one of the main reasons pancreatic cancer is often diagnosed at an advanced stage.
Metastasis: How Pancreatic Cancer Spreads
Once cancer cells gain access to the blood vessels or lymphatic system, they can travel to distant parts of the body and form secondary tumors. This process is called metastasis.
Common sites of metastasis for pancreatic cancer include:
-
The liver: Often the first site of distant spread, due to direct drainage of blood from the pancreas through the portal vein.
-
The lungs: Cancer cells can travel through the bloodstream and lodge in lung tissue.
-
The peritoneum: The lining of the abdominal cavity, where cancer cells can implant and grow.
-
Lymph nodes: Especially those near the pancreas, which serve as a pathway to other parts of the body.
Once metastasis occurs, pancreatic cancer becomes much more difficult to treat and is generally not curable with current therapies.
Why Detection Is So Difficult
One of the key challenges in pancreatic cancer is its silent progression. Tumors can grow and spread for months or even years without producing symptoms.
Several factors contribute to this:
-
Deep anatomical location: The pancreas is hidden behind other organs, making physical exams ineffective.
-
Lack of early symptoms: Digestive changes, weight loss, or pain often appear only after significant tumor growth.
-
No effective screening test: Unlike colon or breast cancer, there is no reliable, routine screening method for average-risk individuals.
-
Rapid disease progression: Once symptoms appear, the cancer often has already advanced beyond the pancreas.
Conclusion
Pancreatic cancer development is a stepwise process that begins with cellular mutations and ends in aggressive invasion and metastasis. It disrupts the pancreas’s normal functions and manipulates the surrounding environment to support its growth and resist immune attack. The disease often advances unnoticed, which is why most patients are diagnosed at a stage when curative treatment is no longer an option.
Improving our understanding of how pancreatic cancer develops is essential to identifying new strategies for early detection, more effective treatments, and ultimately, better patient outcomes. As research continues to explore the genetic, molecular, and environmental factors driving this disease, the hope is that one day pancreatic cancer will no longer be one of the deadliest forms of cancer.

.png)



.png)






